Oregon’s addiction care rollout plan puts peers in a precarious position

On a sunny September evening last year, Nathaniel Sean Stringer joined family and colleagues for a recovery celebration at a park in the eastern Oregon town of Ontario. To enthusiastic applause, he received an award for his service to those struggling with addiction.
Just weeks later, Stringer overdosed on fentanyl and died inside a grocery store. He was 35.

His death shows how fragile recovery from addiction can be — and his story highlights a major pressure point in Oregon’s expanding addiction care system at a pivotal time.
Before he died, Stringer exemplified a growing statewide trend. He worked for the Malheur County Health Department as a peer mentor. “Peers” are people in recovery from addiction who engage with people who use drugs, offering mentorship and resources while demonstrating by example that recovery is possible. There are more than 1,700 peers who specialize in addiction in Oregon, typically earning about $18 to $24 an hour.
The peer model is an evidence-based approach that is increasingly used around the country.
Now, using money generated through Oregon’s 2020 drug decriminalization law, Measure 110, a state-appointed council is pouring money into hiring many more peers as part of a shift toward treating addiction as a health care issue. Increasingly, peers across Oregon are connecting with people in need through street outreach and working in addiction care, mental health or homeless services, hospitals and jails.
But without adequate funding for detox facilities for withdrawal management, residential treatment and recovery housing, people inside the system say the state’s burgeoning peer workforce amounts to a pipeline that often leads nowhere.
A recent analysis from Oregon Health & Science University showed that Oregon’s addiction care system is half the size it should be to meet demand.
Stringer was hired before Measure 110 was implemented, and those close to him believe factors outside his job drove his relapse. What’s clear, however, is that while people in the peer mentor role are tasked with motivating people to seek treatment, they — like Stringer did — frequently grasp for resources that don’t exist when their clients are ready to quit using. The situation puts tremendous stress on the very people on which the system’s current expansion relies.
“I absolutely believe in peers, I believe that they are the best people to engage people who are using drugs into treatment,” said Sarah Poe, director of the Malheur County Health Department, where Stringer worked. But peers don’t themselves provide treatment, and without more services to connect people to, she said, “It’s really hard work for peers to show up and keep trying to push this boulder up a hill — when the hill keeps getting more steep.”
How one peer’s death shook A community
Stringer grew up in Nyssa, a small rural community where both his parents were educators and his grandfather raised sheep. Nyssa sits west of the Idaho border, south of Ontario. In an area known for its crops and cattle, the dusty landscape is dotted with small, well-weathered homes. Malheur County has Oregon’s lowest median income.
Starting with oxycodone as a teenager and then heroin as a college student, Stringer wrestled with addiction for 15 years, going in and out of treatment. His mother, Sherry Stringer, said that one time he vomited before getting into her car after graduating early from an inpatient program. He told her it was because he was afraid of what might come next.
And yet counselors at every treatment center her son went to told her that he was so good at helping others in the program.
“I remember thinking so many times,” she said, “why can’t he help himself?”

Eventually, he did. In 2019, Stringer was a proud father and three years into his recovery as he neared completion of an intensive drug court diversion program. He single-handedly opened a nonprofit syringe exchange to help prevent the spread of disease through intravenous drug use, a need he knew was great. That’s when he connected with health staff at Malheur County for advice on the medical aspects of running an exchange.
County staff were so impressed with Stringer, they later asked if he’d like to work in their new peer support program. He jumped at the opportunity.
In many ways, the job was a perfect fit. His family and friends described him as charismatic, known for his levity. He was empathetic, non-judgmental and defended the underdog. His uncle remembers him in his youth sticking up for a soccer teammate bullied for not being able to afford a uniform.
Stringer was skilled at connecting with clients. Having once contracted Hepatitis C from injecting drugs, he followed-up with county clinic patients who had just tested positive, knowing they likely got it the same way. He let them know he had stopped using and could help them do the same.
A video of him accepting the award last year shows Stringer telling the crowd he loved “every single day” of his job at the county. “The outreach we do is just so important. I get to feel like we are making a difference on the ground, which is what it’s all about.”
But the traits that made him good at his job also added to his stress. His family said it weighed heavily on him when he couldn’t connect his clients to the treatment they needed.
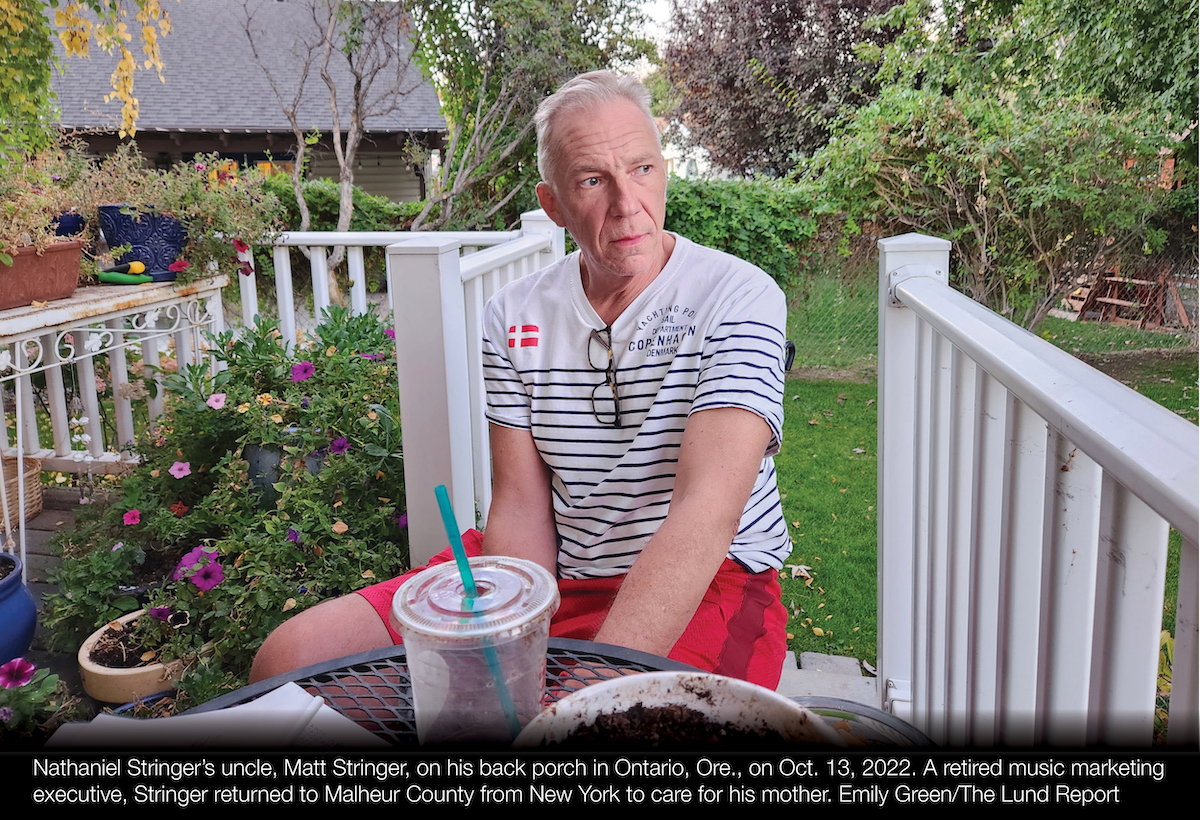
“He was frustrated that there weren’t enough resources,” his uncle, Matt Stringer, said. In the absence of treatment beds, he remembers his nephew considered letting clients stay at his home so they could stop using.
The results of a 2020 statewide survey of Oregon peers indicates the pressure felt by Stringer is mirrored across the state. Participants listed the lack of services for clients as a major challenge, “specifically treatment and housing.”
“When you have two or three or four clients that are needing support right now, and you’re driving them around to each detox center, making phone calls, calling your personal contacts, and then nothing is happening — it’s defeating,” Amanda Esquivel, who has worked as a peer recovery mentor in Portland for the past two years, told The Lund Report in September. “I did that this morning … right now, that individual is waiting at home to get into detox.”
In the weeks leading up to Stringer’s death, his uncle noticed subtle signs that his nephew might not be OK. Pandemic stress and feelings of helplessness around situations with friends and family that were out of his control were climaxing. But he insisted he was fine, colleagues said.
Peers interviewed for this story said it can be hard for people whose jobs are intertwined with their recovery to ask for help when they need it. And peers may fear losing their jobs if they relapse.
Morgan Godvin, a person in recovery who sits on the council implementing Oregon’s drug decriminalization law, is open about this dilemma. If she relapsed, she would “probably hide it,” she said on Twitter. “It would be so profoundly disappointing to everyone who has invested their time and resources in me. I fought really hard to stop being a bitter disappointment. I can’t go back there.”
On Oct. 17, 2021, Stringer went to an Albertsons grocery store not far from Ontario, over the Idaho state line. He walked into the bathroom and consumed a substance containing a fatal amount of fentanyl, his family said.
His family and friends believe it was a momentary lapse.
Stringer left behind a wife of one year, 3-year-old son and a 12-year-old stepson. His death sent waves of shock and grief through eastern Oregon’s recovery community, which included many people he had helped and who looked up to him.
“That’s what broke my heart,” his uncle told The Lund Report. “He was those people’s hope — and then that happens to him?”
Peers are “not A full solution”
Today, a picture of Stringer hangs on a wall in the Malheur County Health Department, outside the door to where his office used to be.
With just 29 staff, the agency is a small operation, located inside a modest one-story office building on the southwest side of Ontario. A rainbow-colored mural spreads across the wall where guests check in at a reception window.
Sarah Poe leads the department. A person in recovery herself, you can hear her passion for her peer support team and their clients as she talks about the high hopes she had for the improvements Measure 110 money could bring to her county — and how those hopes quickly faded.

Measure 110 was sold to voters on the promise of expanding access to drug treatment in a state that ranks highest for its rate of illicit drug use and dead last for its access to treatment, according to federal data.
Following the measure’s passage, however, its proponents have said Measure 110 spending should not focus on residential treatment, arguing that it can be paid for by the Medicaid-funded Oregon Health Plan.
This change has come as a blow to providers who thought much of the measure’s $300 million would go to expanding treatment infrastructure, then watched as the council that oversees Measure 110 spending rejected applications for stabilization centers, residential treatment and detox facilities.
Even with recent increases in reimbursements, Medicaid doesn’t come close to covering the full cost of treatment. That’s why Heather Jefferis, executive director of Oregon Council For Behavioral Health, calls addiction care in Oregon “the most extreme example of how historic underfunding creates tragic outcomes.”
Providers also need money to purchase or erect the buildings that will house needed services to begin with. The Legislature’s recent investments in behavioral health care have largely gone to mental health, not addiction treatment. And, there’s no plan for investing in the level of detox beds, residential treatment or housing for people in outpatient treatment that would be required to meet demand.
The frustration is evident statewide, and especially in Malheur County.
“We got all this money that came into our community, and you know what it gave us? More peers, more syringe exchanges, more Narcan,” Poe said, referring to an opioid overdose-reversing drug. These services are critical, she said, but on their own, “they’re not a full solution. And we really, really, really needed a detox facility.”
Poe wondered aloud why the state isn’t taking steps to ensure each region has the basic building blocks of a functioning treatment system in place: a detox center for withdrawal management, an overdose prevention coordinator, sufficient residential treatment, recovery housing and other baseline necessities.

In Malheur County, Poe said she’s watching as health department peers hand out more and more Narcan so that people using heroin and opioids can reverse potentially-fatal overdoses.
“Narcan is just there to keep someone alive to then get them into the treatment that they need,” Poe said. “But then we need to have the treatment piece there.”
Peers bear the weight of a broken system
Janie Gullickson fought through methamphetamine addiction before becoming the director of the state’s most prominent peer-run organization, the Mental Health & Addiction Association of Oregon. Her enthusiasm is infectious when she speaks about the strength and resiliency of the peers she represents. As one of Measure 110’s chief petitioners, she believes in the law and its role in “expanding addiction recovery services across the continuum.”
Working out of her nonprofit’s headquarters in Northeast Portland, Gullickson oversees training, supervision and support for peers around Oregon — including in state-supported programs like Stringer’s in Malheur County.

Gullickson told The Lund Report that the recovery community in Oregon has seen an increase in relapses and overdoses during the pandemic, including among peers like Stringer.
In the wake of Stringer’s death, the health authority began requiring more structure to supervisory support for peers in state-funded peer programs, though a state spokesperson denied any connection between the two.
And for county-based peer programs that wanted outside help, the state also provided supervision and support by contracting with Gullickson’s organization.
“Some had great, experienced peer supervisors and were already doing peer programs. But it was those ones that felt very isolated and didn’t have that infrastructure that we focused on,” Gullickson said. They also worked with Malheur County, where the peer supervisor had been Stringer and his replacement was a member of his team, she said.
According to a statewide assessment Gullickson’s nonprofit helped conduct in 2020, fewer than half of peers reported receiving supervision once a week or more. Some participants attributed high turnover to a lack of support, trauma and burnout.
But Gullickson said it’s important not to “other” peers by suggesting they need more supervision than other workers and suggested stigma may play a larger role than supervision in relapse.
“What we’ve seen sometimes is people won’t say, ‘Hey, I need help right now’ in the way that we would think people in recovery would be able to do. But when they get in this profession, often then it’s like, ‘Oh, I’ve got to prove myself.’”
Before 2020, the state required that peers have at least two years of recovery behind them before taking the 40- or 80-hour certification courses. To meet the demand for peers and behavioral health counselors, authorities lowered the requirement to one year.
Adding to the stress of their job, many peers also say that the residential programs currently used in Oregon need to offer longer stays and different approaches to increase their effectiveness.
Kevin Fitts, a peer and director of the Oregon Mental Health Consumers Association, told a crowd during the recent opening of Multnomah County’s Behavioral Health Resource Center that while the focus now is addressing the extreme shortages in behavioral health, the question that’s being neglected is whether the current model for treatment is succeeding.
“Are we having beneficial outcomes for the consumer of the services? Got me!” Fitts said. “We have a system in crisis. … What is important is getting the services that these people need out on the street. Well, are these services meeting the needs? Are people moving forward?”
Dreams dashed in Ontario
On a Thursday morning in September, the smell of homemade meatloaf filled the air inside a mid-century brick church on the northwest side of Ontario.
Steven Wolf greeted patrons as they walked up to the back door. Wolf is a peer mentor, a job that Stringer recruited him into. The two graduated from drug court together before becoming peers.
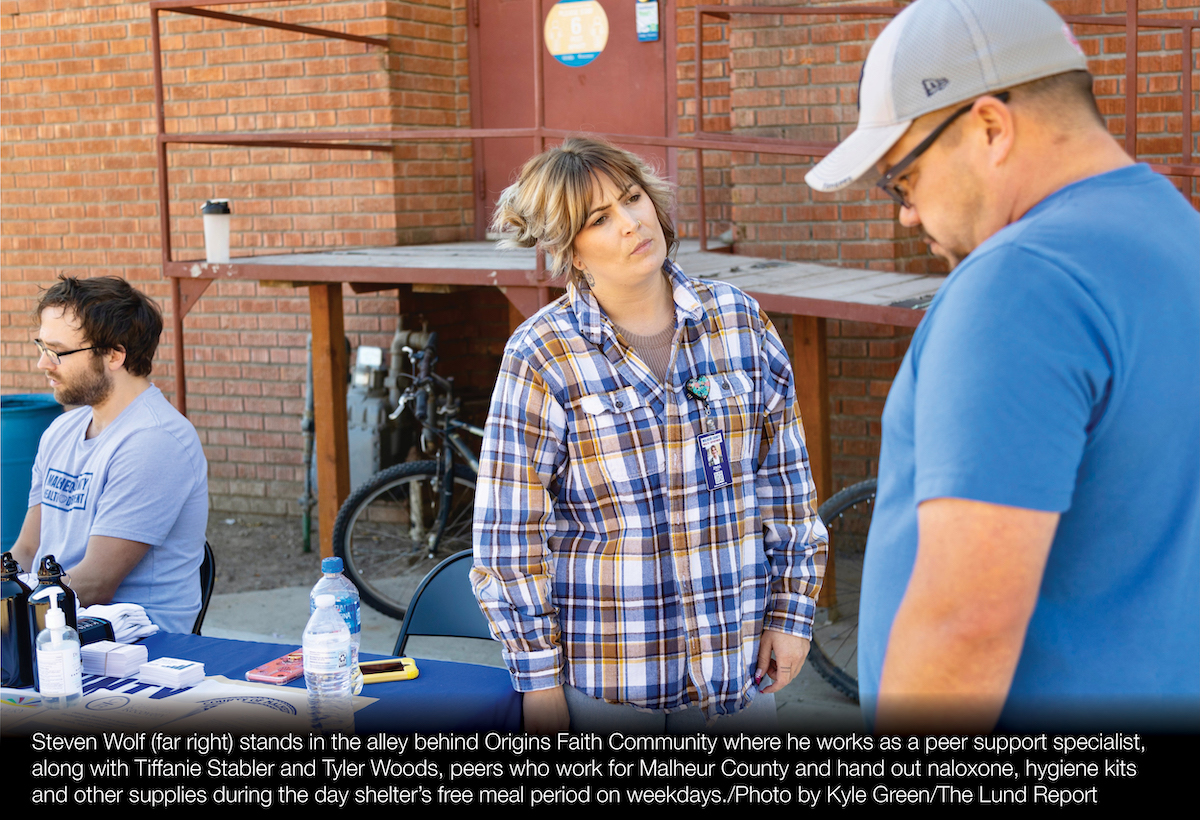
Like most mornings, Anthony Caliendo, 52, was the first to show up. He’s experienced homelessness since July. He told The Lund Report he’s not interested in drug treatment. But Wolf said he helped Caliendo rely more on cannabis and less on meth — a harm reduction method employed by some peers.
Caliendo said Wolf is easy to talk to because he comes from a similar background. “He’s been hungry and spent his money on dope instead of food,” he said.
With no local year-round homeless shelter in the area, the church is the only place in Ontario where people can get a free meal. No longer operating as a house of worship, the building serves as a drop-in center run by a small nonprofit called Origins Faith Community, which is not religiously affiliated.
Staff at Origins saw Measure 110 as the opportunity they had been waiting for. They launched a peer program with Measure 110 funds, and hired Wolf as its first peer.
But as the state program unfolded, it became clear that the robust local system Origins and other local providers had planned was not going to be possible.
Origins originally asked the Measure 110 council for $3.1 million. But the state wouldn’t fund the requested transportation services, new drop-in center, and the purchase of a 20-unit apartment building adjacent to the church.
Altruistic Recovery, an outpatient behavioral health clinic across town, requested $13 million to create a detox and residential treatment facility, but was also denied.
Of the $265 million in funds distributed through Measure 110 this year, $1.8 million went to Malheur County.
That money, locals lament, will fund only seven beds — slated for an apartment complex that a local nonprofit plans to purchase as housing for people living with co-occurring HIV and substance use disorder.

Origins, meanwhile, got $616,000 — less than 20% of what it hoped for.
Counselor Dana Rush, who left Origins following cuts made in November, said she thought that Measure 110 was going to be different.
“That’s why we were so excited about it — that finally, we could really meet people where they were,” she said, her voice breaking as tears filled her eyes. “And then to watch all of the stuff unfold and go, ‘Oh my gosh, we’re not going to be able to do that. OK, give us just what you can so we can just get started. And maybe we can build what we can. And we’ll do what we can. And we’ll keep doing what we can until — dang it — we’re just gonna keep doing what we can do.’”
In memory of Nathaniel Sean Stringer, Four Rivers Healthy Community is raising funds for a scholarship to Treasure Valley Community College for people in recovery, as well as a memorial tree and bench.
This story was originally published in The Lund Report and is reprinted with permission.
The Lund Report is tracking addiction issues as part of a reporting fellowship sponsored by the Association of Health Care Journalists and The Commonwealth Fund. Emily Green can be reached at [email protected].
STORY TIP OR IDEA? Send an email to Salem Reporter’s news team: [email protected].
JUST THE FACTS, FOR SALEM – We report on your community with care and depth, fairness and accuracy. Get local news that matters to you. Subscribe to Salem Reporter. Click I want to subscribe!